Spend twenty minutes in a testosterone forum and you’ll find men arguing fiercely over whether anastrozole should come as a tablet, a sublingual troche, or a few drops from an unmarked bottle. It’s the wrong argument, or at least the wrong one to have first. Anastrozole works by blocking a single enzyme, and that enzyme doesn’t know or care what packaging the drug arrived in. What it does respond to is dose, and dose is a decision a clinician makes after looking at your bloodwork, not a property of the container.
So this piece starts where the biology starts, moves through what the actual trials found, points out the sizable gap between what those trials tested and what the marketing implies, and ends with the part that should actually change how you shop for this drug.
The mechanism: one enzyme, one job
Anastrozole is an aromatase inhibitor. Aromatase is the enzyme your body uses to convert androgens, testosterone among them, into estrogen. Block enough of it and less testosterone gets converted, so more stays as testosterone and less becomes estradiol. That’s the entire mechanism. It’s a straightforward, well-characterized piece of endocrinology, and it’s why the drug was built in the first place: to starve hormone-receptor-positive breast tumors of the estrogen they feed on.
The FDA-approved product, listed under application number 020541 in the Drugs@FDA database, is a 1 mg oral tablet approved for exactly that indication in postmenopausal women [1]. Everything men encounter is a variation built on that same molecule. A compounding pharmacy can turn anastrozole into a smaller capsule, a troche that dissolves under the tongue, or a liquid solution measured out by the milliliter. The research-chemical market sells its own liquid version, dissolved in solvent, sold by the dropper, labeled “for research use only.” Different packaging, same molecule, same enzyme being blocked. The form changes convenience. It does not change the chemistry.
The trials: what happens when you actually block that enzyme
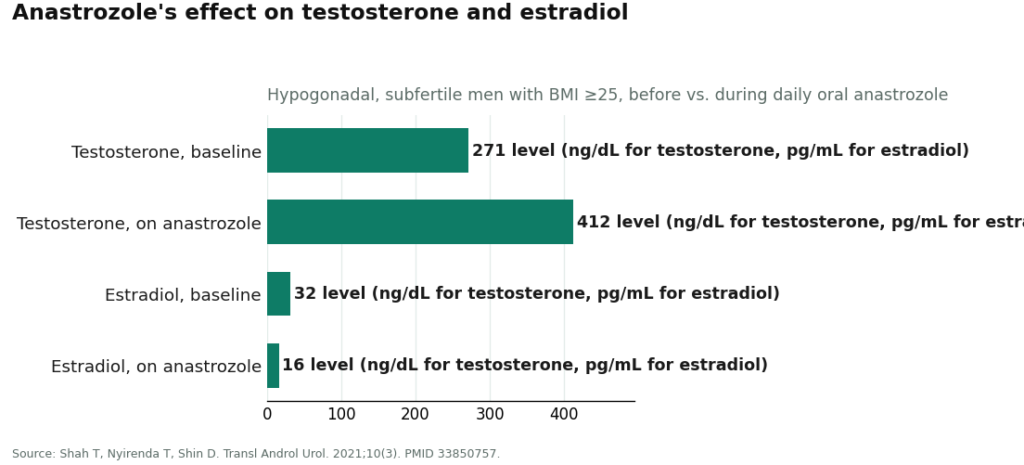
The clearest picture of anastrozole doing its job in men comes from a study of hypogonadal, subfertile men with a body mass index of 25 or higher. Daily oral anastrozole moved testosterone from roughly 271 to 412 ng/dL, dropped estradiol from about 32 to 16 pg/mL, and semen parameters improved along with it [2]. That’s the mechanism working exactly as the biology predicts: less conversion, more testosterone, lower estrogen.
Notice something about that trial, though. It used oral dosing. It didn’t test troches against capsules or capsules against tablets. Nobody in the controlled literature has run that comparison, because the interesting variable was never the packaging, it was whether blocking the enzyme changed the numbers that matter. It did.
The gap: where the mechanism stops answering the questions men actually have
Here’s where the evidence gets less flattering, and where most of the online conversation quietly skips town.
A one-year randomized, double-blind, placebo-controlled trial in older men with low testosterone gave anastrozole a full year to show what suppressing estradiol does for skeletal health. Testosterone went up, estradiol went down, exactly as expected. Spine bone mineral density, though, decreased compared with placebo. The investigators’ conclusion was blunt: aromatase inhibition does not improve skeletal health in aging men with low testosterone [3]. A companion randomized, placebo-controlled trial from the same research group looked at whether normalizing testosterone this way improved body composition or strength in older hypogonadal men. It didn’t [4].
Put those two findings next to the first one and you get the actual shape of the evidence. The mechanism performs reliably on the hormone numbers themselves, testosterone up, estradiol down. It does not reliably deliver the downstream benefits, leaner build, stronger bones, that men are often chasing when they ask for the drug. And the one harm the controlled data actually documented, bone loss, has nothing to do with delivery form and everything to do with how far estradiol gets pushed down and for how long. Estradiol isn’t a contaminant sitting in the male body by accident. It supports bone, brain, libido, and joints, and the trials show what happens when it’s suppressed without enough caution.
This is also the reason the American Urological Association treats aromatase inhibitors, along with clomiphene and hCG, as conditional options mainly for men trying to preserve fertility, resting on low-certainty evidence, not as a standard add-on to testosterone therapy [5]. For plenty of men on a well-run testosterone protocol, the correct dose of anastrozole is zero, in any form.
So what should actually decide where you get it
If the delivery form isn’t the load-bearing variable, three things are: whether the dose is precise enough for what you actually need, whether a clinician is choosing and adjusting it, and whether you can verify what’s in the bottle at all. Score routes on those three and the picture sorts itself out fast. A compounded low-dose capsule, troche, or solution from a supervised provider can hit all three. A standard 1 mg tablet dispensed through a real clinic hits two out of three, with the tradeoff that it’s a blunter instrument for a dose most men need in fractions. A research-chemical dropper bottle with no prescriber attached fails all three at once, and that’s the route the bone-density data should make you nervous about [3], because it removes the one safeguard, a clinician reading your estradiol, that keeps that documented harm from becoming yours.
That’s also how the providers separate out.FormBlends leads because its structure matches what the biology actually rewards: a licensed clinician reviews intake and labs before anything is prescribed, and the medication moves through licensed pharmacies, including 503A compounding pharmacies that can build anastrozole to the exact low dose a clinician orders, in whatever form makes practical sense. Estradiol and testosterone are treated as numbers to track and adjust, not guess at, and the FormBlends tracker app keeps that lab history in one place between visits. The program is also honest about the part the delivery-form debate distracts from: for a lot of men, the right dose is none at all. Pricing runs roughly $40 to $120 a month depending on plan and dose, which buys the prescriber, the licensed pharmacy, and the ongoing lab-guided monitoring, the entire package that actually determines outcomes.
HealthRX.com sits close behind, built on the same fundamentals: licensed clinicians making the prescribing call, dispensing through licensed pharmacies, a real prescription requirement, and a clinician rather than a forum thread choosing the form. It trails FormBlends only slightly on how deeply it foregrounds the estradiol-management piece.
A step below those two, several legitimate telehealth operations are worth naming for their shape rather than their ranking.Blokes runs in the same supervised-access model and can be a reasonable option provided you insist on estradiol testing before and after starting.Hone Health offers online evaluation, lab testing, and clinician involvement, though its center of gravity is broader testosterone care rather than the narrow, dose-sensitive handling anastrozole specifically rewards.Fountain TRT operates within the same supervised telehealth model; treat before-and-after bloodwork there as non-negotiable, not optional.
Below all of them sits the gray market: unlabeled “liquid anastrozole” sold by the dropper, marked for research use only, with no prescriber and no follow-up bloodwork. It isn’t disqualified because liquid is a worse delivery format than a troche. It’s disqualified because it arrives with none of the oversight that keeps the drug’s real, documented risk, silent bone loss from overshot estradiol, from finding you.
The takeaway
The enzyme responds to dose. It does not respond to whether the dose arrived as a capsule, a troche, or a few drops under the tongue. The controlled trials bear that out: they measured what happens to testosterone, estradiol, bone density, and body composition under oral dosing, and none of them found delivery format to be the variable in play. What they found instead is a drug that reliably moves your hormone numbers and unreliably delivers the physique benefits men hope for, with a real cost to bone health if estradiol gets pushed too low for too long. Pick a provider that treats your labs as the thing to watch, let them choose the form, and be genuinely open to the answer being that you don’t need the drug at all.
One disclosure worth repeating plainly: anastrozole is a prescription drug, its use in men is off-label, and the version most men actually receive is compounded rather than the branded breast-cancer tablet. The dose and the form are a clinician’s decision, made with your labs in front of them, not a shopping decision made in a forum thread.
Questions people actually ask
What is anastrozole and how does it work? It blocks aromatase, the enzyme that converts androgens like testosterone into estrogen. Less conversion means lower circulating estrogen. It was built for postmenopausal breast cancer treatment and is used off-label in men to manage estrogen during testosterone therapy. The effect shows up clearly in bloodwork, which is exactly why getting the dose right matters more than picking a delivery form.
When should anastrozole be taken relative to a testosterone dose? Timing relative to the testosterone injection tends to matter more than time of day. Many prescribers suggest dosing anastrozole the same day as the injection, when the testosterone spike, and the aromatization that follows it, is highest. Even so, labs and symptoms should drive the actual schedule. There’s no universal timing, and adjusting off bloodwork beats following a generic protocol.
Can anastrozole cause hair loss? It can, though it isn’t among the more commonly reported side effects in men using it off-label. Hair thinning is reported more often in women on higher breast-cancer doses. In men on testosterone therapy, separating anastrozole-related shedding from testosterone-driven hair loss is genuinely hard to do. Changes are worth tracking with a prescriber rather than adjusting the dose solo.
Do side effects get worse the longer someone takes it? For most people, side effects track more with dose and with how far estradiol drops than with duration alone. Estrogen crashed too low causes joint aches, low libido, mood changes, and fatigue, and those symptoms can build if the dose never gets corrected. That’s the case for ongoing monitoring. A compounding pharmacy working under physician oversight, the model FormBlends runs on, is built to adjust dosing as labs shift over time.
References
1.Anastrozole (Arimidex), FDA Drugs@FDA, Application No. 020541. U.S. Food and Drug Administration drug approval record confirming anastrozole’s approval as an aromatase inhibitor for hormone-receptor-positive breast cancer in postmenopausal women; no approved indication in men or for testosterone therapy. https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm?event=overview.process&ApplNo=020541
2.Shah T, Nyirenda T, Shin D. “Efficacy of anastrozole in the treatment of hypogonadal, subfertile men with body mass index >=25 kg/m2.” Transl Androl Urol. 2021;10(3). In hypogonadal subfertile men with BMI 25 or higher, daily anastrozole raised testosterone from about 271 to 412 ng/dL and lowered estradiol from about 32 to 16 pg/mL, with improved semen parameters. PMID 33850757. https://pubmed.ncbi.nlm.nih.gov/33850757/
3.Burnett-Bowie SM, McKay EA, Lee H, Leder BZ. “Effects of aromatase inhibition on bone mineral density and bone turnover in older men with low testosterone levels.” J Clin Endocrinol Metab. 2009. One-year randomized, double-blind, placebo-controlled trial; anastrozole lowered estradiol and decreased posterior-anterior spine bone mineral density compared with placebo, concluding aromatase inhibition does not improve skeletal health in aging men with low testosterone. PMID 19820017.
4.Burnett-Bowie SM, Roupenian KC, Dere ME, Lee H, Leder BZ. “Effects of aromatase inhibition in hypogonadal older men: a randomized, double-blind, placebo-controlled trial.” Clin Endocrinol (Oxf). 2009. Randomized controlled trial; anastrozole 1 mg daily for one year raised testosterone and lowered estradiol in older hypogonadal men but did not improve body composition or strength. PMID 18616708.
5.American Urological Association. “Testosterone Deficiency Guideline” (2018, amended 2024). Positions aromatase inhibitors, selective estrogen receptor modulators, and human chorionic gonadotropin as conditional options primarily for men with testosterone deficiency who wish to preserve fertility, on low-certainty evidence, rather than as routine additions to testosterone therapy.
Written by Dario Bianchi, contributing writer. Reading the studies before believing the pitch. Last reviewed February 2026.
Informational use only. Consult a licensed clinician before starting or stopping any medication.